28 Feb 2020
Coronary sinus reducer for microvascular angina
Supported by the EuroIntervention Journal
A 61-year-old man with a history of 2-vessel coronary artery stenting, hypertension and type-2 diabetes mellitus was admitted 5 times within September 2017 and November 2018 for recurrent angina CCS class III-IV refractory to therapy with nitrates, b-blockers and ranolazine in maximally tolerated doses...
Author
Case summary
A 61-year-old man with a history of 2-vessel coronary artery stenting, hypertension and type-2 diabetes mellitus was admitted 5 times within September 2017 and November 2018 for recurrent angina CCS class III-IV refractory to therapy with nitrates, b-blockers and ranolazine in maximally tolerated doses.
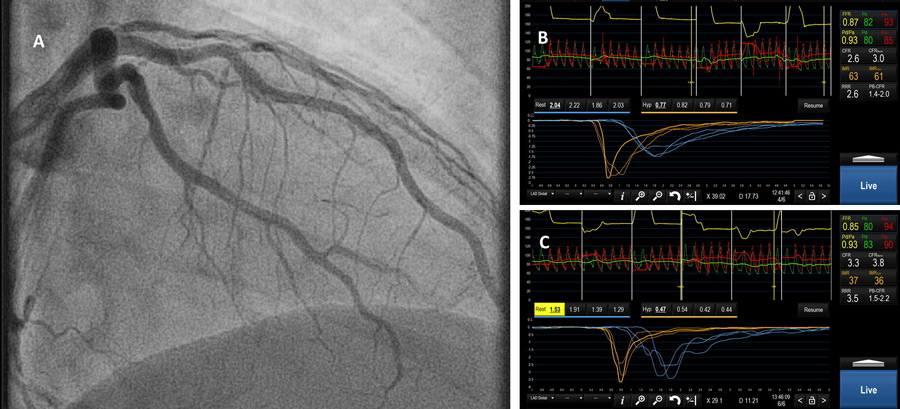
Panel A: Angiography
Panel B: Resting assessment of coronary hemodynamics
Panel C: Post-Reducer Implant Physiology
Coronary angiography and fractional flow reserve excluded the presence of epicardial stenosis (Panel A). ECG during angina attacks showed anterolateral ST-segment depression. The cardiac microcirculation was investigated (Panel B) with coronary flow reserve, which was mildly depressed (2.6, normal above 3) and the index of microvascular resistance (Abbott, Santa Clara, USA and Coroventis, Sweden), which was markedly pathologic (63, normal values below 25).
Based on this evidence of microvascular ischemia, a coronary sinus reducer (Neovasc, Vancouver, Canada) was implanted. Immediately following implantation, a pressure gradient of 4mmHg could be measured across the device. This was associated with a marked improvement in coronary flow reserve (3.3) and the index of microvascular resistance (37, Panel C).
The patient is asymptomatic since March 2019.
Evidence from animal studies demonstrates that coronary sinus obstruction leads to an increase in retrograde pressure, resulting in redistribution of myocardial blood flow from epicardial to ischemic endocardial layers[1], which might have produced the decrease in overall coronary resistance observed here. In a sham-controlled randomized trial[2], the coronary sinus reducer has been shown to improve symptoms in patients with refractory angina and no revascularization option, and preliminary evidence suggests that a similar effect might also hold for patients without epicardial disease[3]. The mechanism causing the acute gradient in a non-endothelialized device is unclear, but flow turbulences or the implantation on a venous valve could be advocated as possible explanations. The current case confirms that sinus reduction might be a possible approach for microvascular angina, a frequent condition for which no appropriate therapy has been developed yet.
Conflict of interest statement
T. Gori has received honoraria from Neovasc and Abbott vascular.
Affiliations
- Kardiologie I, Universitätsmedizin Mainz, and DZHK Standort Rhein-Main, Germany
References
- Ido A, Hasebe N, Matsuhashi H and Kikuchi K. Coronary sinus occlusion enhances coronary collateral flow and reduces subendocardial ischemia. Am J Physiol Heart Circ Physiol. 2001;280:H1361-7.
- Verheye S, Jolicoeur EM, Behan MW, Pettersson T, Sainsbury P, Hill J, Vrolix M, Agostoni P, Engstrom T, Labinaz M, de Silva R, Schwartz M, Meyten N, Uren NG, Doucet S, Tanguay JF, Lindsay S, Henry TD, White CJ, Edelman ER and Banai S. Efficacy of a device to narrow the coronary sinus in refractory angina. N Engl J Med. 2015;372:519-27.
- Giannini F, Baldetti L, Ielasi A, Ruparelia N, Ponticelli F, Latib A, Mitomo S, Esposito A, Palmisano A, Chieffo A and Colombo A. First Experience With the Coronary Sinus Reducer System for the Management of Refractory Angina in Patients Without Obstructive Coronary Artery Disease. JACC Cardiovasc Interv. 2017;10:1901-1903.
1 comment
nice case ,good demonstration